
Diabetic Retinopathy
Page Menu
Introduction to Diabetic Retinopathy
How Diabetes Affects the Retina
Non-Proliferative Diabetic Retinopathy
Proliferative Diabetic Retinopathy
Diabetic Macular Oedema (DMO)
Importance of Regular Eye Examinations
Retinal Imaging and Diagnostic Technology
Optical Coherence Tomography (OCT)
Ultra-Widefield Retinal Imaging
Ultra Wide-field Fluorescein Angiography
Long-Term Management of Diabetic Eye Disease
Fenofibrate and Diabetic Retinopathy
Diabetic Retinopathy Assessment in Sydney
Introduction to Diabetic Retinopathy
Diabetic retinopathy is one of the leading causes of vision impairment in working-age adults and remains a major complication of both type 1 and type 2 diabetes. The condition develops when chronically elevated blood glucose levels damage the delicate retinal blood vessels at the back of the eye. Over time, these vascular changes may lead to retinal haemorrhage, fluid leakage, retinal swelling, oxygen deprivation and abnormal new blood vessel growth. If severe, diabetic retinopathy can cause severe vision impairment, meaning patients no longer meet the driving standards in Australia to maintain their driving licence. Drivers have a legal responsibility to inform the licencing authority.
One of the challenges of diabetic eye disease is that significant retinal damage may occur before patients notice obvious visual symptoms. Some patients maintain relatively good vision despite advanced retinal pathology, while others may develop sudden visual deterioration from diabetic macular oedema or vitreous haemorrhage. Regular retinal examination and imaging therefore play a critical role in detecting diabetic retinopathy before permanent vision loss occurs.
Modern diabetic retinopathy management has evolved substantially over the past two decades. Advanced retinal imaging, optical coherence tomography (OCT), intravitreal anti-VEGF injections, retinal laser treatment and vitreoretinal surgery have significantly improved outcomes for many patients. However, diabetic retinopathy remains a chronic disease that often requires long-term monitoring and ongoing care.
At Eye and Retina Specialists, diabetic retinal disease is assessed using detailed retinal examination and advanced imaging technologies including OCT and wide-field retinal imaging. Management may involve observation, retinal laser treatment, intravitreal eye injections or vitreoretinal surgery depending on the stage and severity of disease.

Retinal photographs demonstrating bilateral non proliferative diabetic retinopathy with scattered haemorrhages, microaneurysms and hard exudates
How Diabetes Affects the Retina
The retina is a highly specialised layer of neural tissue lining the back of the eye. It relies on a complex network of tiny blood vessels to supply oxygen and nutrients. In patients with diabetes, persistently elevated blood glucose levels can gradually damage these small retinal blood vessels through multiple mechanisms including endothelial dysfunction, chronic inflammation, oxidative stress and impaired vascular autoregulation.
Early diabetic retinal disease is characterised by weakening of the capillary walls and breakdown of the blood-retinal barrier. Tiny outpouchings known as microaneurysms may develop, allowing leakage of fluid, lipids and blood into the retina. As the disease progresses, retinal capillaries may close completely, reducing oxygen delivery to retinal tissue.
In response to retinal ischaemia, the eye produces increased levels of vascular endothelial growth factor (VEGF), a signalling protein that promotes abnormal blood vessel growth and vascular leakage. Although VEGF initially represents the retina’s attempt to compensate for reduced oxygen supply, excessive VEGF activity contributes to diabetic macular oedema and proliferative diabetic retinopathy.
Importantly, these changes may progress silently for years. Many patients with moderate or even severe diabetic retinopathy continue to read well and remain asymptomatic until the macula becomes involved or complications such as vitreous haemorrhage occur.
Non-Proliferative Diabetic Retinopathy (NPDR)
Non-proliferative diabetic retinopathy (NPDR) represents the earlier stages of diabetic retinal disease and is commonly classified as mild, moderate or severe.
In mild diabetic retinopathy, retinal examination may reveal scattered microaneurysms and small retinal haemorrhages. As disease severity increases, additional features may develop including:
-
worsening intraretinal haemorrhages
-
cotton wool spots
-
venous beading
-
intraretinal microvascular abnormalities (IRMA)
-
lipid exudates
Severe NPDR indicates substantial retinal vascular compromise and carries a significantly increased risk of progression to proliferative diabetic retinopathy.
One of the important clinical features of NPDR is the often poor correlation between retinal appearance and visual symptoms. Some patients with advanced retinal pathology continue to function visually quite well, particularly if the macula remains relatively spared. This is one reason why routine diabetic retinal examination remains important even when vision appears “normal”.
Proliferative Diabetic Retinopathy (PDR)
Proliferative diabetic retinopathy (PDR) represents advanced diabetic retinal disease and develops when widespread retinal ischaemia stimulates the formation of abnormal new blood vessels. These vessels, known as retinal neovascularisation, are fragile and prone to bleeding. Unlike normal retinal vasculature, they lack structural stability and may grow along the retinal surface, optic disc or into the vitreous cavity.
Patients may experience sudden onset floaters, haze or severe visual loss from vitreous haemorrhage. In more advanced disease, scar tissue associated with neovascularisation may contract and pull on the retina, resulting in tractional retinal detachment.
Complications of proliferative diabetic retinopathy may also lead to:
-
recurrent vitreous haemorrhage
-
severe retinal fibrosis
-
combined tractional/rhegmatogenous retinal detachment
-
neovascular glaucoma
-
irreversible vision loss
Unlike earlier stages of diabetic retinopathy, proliferative disease usually requires reasonably urgent treatment to reduce the risk of major visual complications and severe visual loss. This can be in the form of extensive retinal laser to the peripheral retina known as panretinal photocoagulation (PRP). Evidence has emerged on the use of intravitreal anti-VEGF eye injections in the management of proliferative diabetic retinopathy. Studies have shown that compared to panretinal photoagulation laser, intravitreal anti-VEGF injections may be associated with improved peripheral vision and night vision. However regular injections are needed and strong patient compliance required to prevent more serious worsening if the injections are suddently stopped.
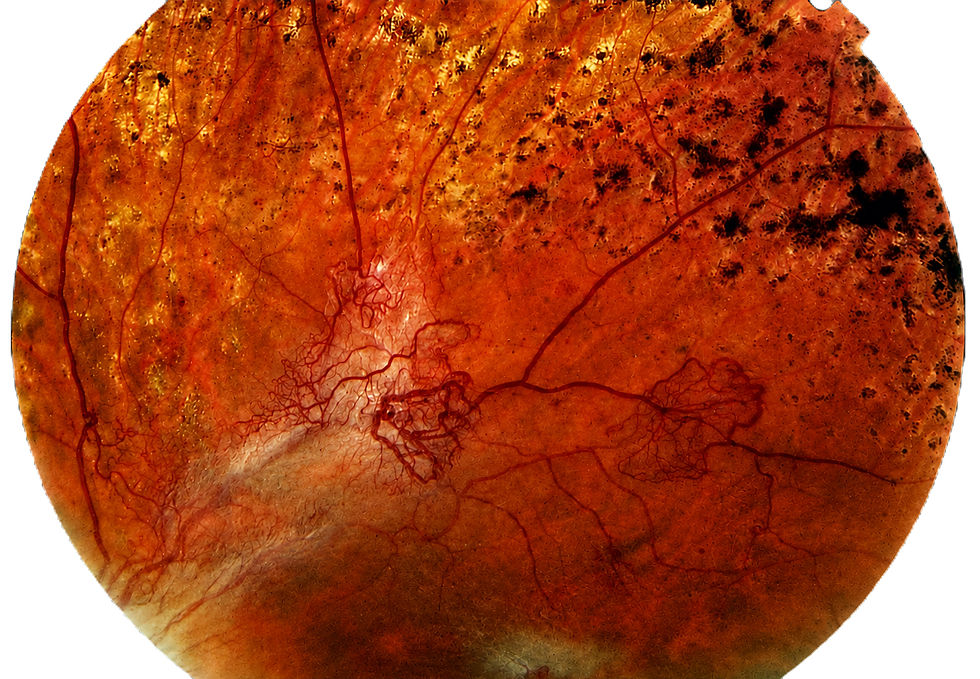
Retinal photograph demonstrating proliferative diabetic retinopathy with new retinal blood vessels (neovascularisation) and retinal laser

Retinal photograph showing proliferative diabetic retinopathy with subhyaloid haemorrhage threatening central vision
Diabetic Macular Oedema (DMO)
Diabetic macular oedema (DMO) is one of the most important causes of vision impairment in patients with diabetic eye disease and may develop in both non proliferative and proliferative diabetic retinopathy. The macula is the central part of the retina responsible for detailed vision required for reading, driving and recognising faces. When damaged retinal blood vessels begin to leak fluid into the macula, cystic fluid accumulation may develop, disrupting normal retinal architecture and impairing central vision.
Some patients describe gradually increasing blur or difficulty reading, while others notice distortion, fluctuating visual quality or increasing glare sensitivity. In certain cases, vision may remain surprisingly good despite significant retinal swelling demonstrated on imaging. Conversely, relatively subtle oedema affecting the fovea may produce marked visual symptoms.
Optical coherence tomography (OCT) has become central to modern diabetic macular oedema management. OCT imaging provides detailed cross-sectional visualisation of the retina and can identify intraretinal fluid, cystic change and retinal thickening that may not yet be obvious on clinical examination alone. OCT also allows careful longitudinal monitoring of disease activity and treatment response over time.
First line treatment for diabetic macular oedema is intravitreal eye injection therapy of anti-VEGF medication. Treatment usually starts with an initial loading phase of monthly injections for the first six months. Following the initial treatment phase, management is individualised depending on the response to treatment.
Some patients with persisting diabetic macular oedema may benefit from an intravitreal slow release steroid medication in the eye. Focal and macular grid laser is less common than previously done, but can still have an adjunctive role in some patients.

Sequential OCT imaging demonstrating progressive improvement in diabetic macular oedema following intravitreal anti-VEGF treatment
Importance of Regular Diabetic Eye Examinations
One of the major challenges in diabetic eye disease is that retinal damage may progress silently for years before patients become aware of visual symptoms. Significant diabetic retinopathy can therefore be present even in patients who feel their vision is relatively normal.
Patients with type 2 diabetes may already have established diabetic retinopathy at the time of diagnosis because elevated blood glucose levels often precede formal diagnosis by many years. In patients with type 1 diabetes, the likelihood of diabetic retinal disease increases progressively with disease duration. Pregnancy may also accelerate diabetic retinopathy progression in some people particularly in those with pre-existing retinal disease.
Regular retinal examination allows earlier detection of retinal haemorrhage, diabetic macular oedema, retinal ischaemia and proliferative disease before irreversible visual loss occurs.
Long-term diabetic retinal management is also affected by systemic factors, especially glycaemic (sugar) control, blood pressure control and smoking
Retinal Imaging and Diagnostic Technology
Modern diabetic retinal management relies heavily on retinal imaging, both for diagnosis and for long-term monitoring of disease activity over time. Imaging technologies now allow subtle retinal changes to be detected far earlier than was previously possible and provide important information regarding retinal structure, vascular leakage and retinal perfusion.
Optical Coherence Tomography (OCT)
Optical coherence tomography has transformed the management of diabetic macular oedema and is now routinely used during diabetic retinal assessment. OCT provides high-resolution cross-sectional imaging of the retina and allows precise visualisation of retinal thickening, intraretinal cystic change and subretinal fluid.
At Eye and Retina Specialists, serial OCT imaging is used to monitor changes in retinal thickness, intraretinal fluid and treatment response over time. Careful comparison between visits may help identify subtle progression or recurrence of diabetic macular oedema and assist in individualising treatment intervals during ongoing anti-VEGF therapy.
Ultra-Widefield Retinal Imaging
Ultra-widefield retinal imaging allows visualisation of far more peripheral retina than conventional retinal photography and has become increasingly valuable in the assessment of diabetic retinal disease, particularly proliferative diabetic retinopathy.
In many patients, substantial retinal pathology extends well beyond the posterior pole. Peripheral retinal haemorrhages, capillary non-perfusion and retinal neovascularisation may be more clearly appreciated on ultra-widefield imaging and can contribute significantly to understanding overall disease severity.
Serial ultra-widefield imaging also provides valuable documentation during long-term follow-up, allowing retinal changes to be compared across multiple visits and assisting in treatment planning, particularly when panretinal photocoagulation laser is being considered.

Ultra-widefield retinal imaging demonstrating extensive panretinal photocoagulation (PRP) laser treatment for proliferative diabetic retinopathy
Ultra-Widefield Fundus Fluorescein Angiography
Ultra-widefield fluorescein angiography is an important investigation in patients with diabetic eye disease when there are concerns regarding retinal ischaemia and proliferative diabetic retinopathy.
During fluorescein angiography, a fluorescent dye is injected intravenously and sequential retinal photographs are obtained as the dye circulates through the retinal vasculature. The investigation is important to detect retinal ischaemia, leaking diabetic microvascular aneurysms and proliferative retinopathy. This information is important in guiding ongoing best management of the diabetic retinopathy.

Ultra-widefield retinal image showing areas of laser panretinal photocoagulation in diabetic retinopathy

Ultra-widefield fluorescein angiography of the same eye demonstrating multiple areas of leakage consistent with proliferative diabetic retinopathy
Long-Term Management of Diabetic Eye Disease
Diabetic retinopathy is often a chronic condition requiring ongoing monitoring over many years. Although modern retinal treatments have significantly improved outcomes for many patients, successful management depends not only on retinal procedures and imaging, but also on long-term diabetic control and regular follow-up.
At Eye and Retina Specialists, diabetic retinal care is tailored to the individual patient and may involve serial OCT imaging, ultra-widefield retinal photography, fluorescein angiography, retinal laser treatment and intravitreal injection therapy depending on the severity and behaviour of the disease over time.
Importantly, many patients with diabetic retinopathy maintain useful vision for many years with appropriate monitoring and timely treatment. Early detection remains critical, as diabetic retinal disease often progresses silently before noticeable visual symptoms develop.
Management of diabetic eye disease is often best approached collaboratively alongside the patient’s general practitioner, endocrinologist, diabetes educator and dietitian, particularly where optimisation of blood glucose levels, blood pressure, cholesterol and overall vascular risk factors may influence long-term retinal outcomes.
Patients with diabetes should seek prompt assessment if they experience:
-
sudden visual deterioration
-
distorted central vision
-
increasing blurred vision
-
loss of peripheral vision
Even in the absence of symptoms, regular diabetic retinal examination remains important.
Fenofibrate and Diabetic Retinopathy
Fenofibrate has been investigated extensively in diabetic retinal disease following large randomised clinical trials demonstrating reductions in diabetic retinopathy progression and reduced need for retinal laser treatment in selected patients with type 2 diabetes and pre-existing diabetic retinopathy. In the FIELD study, patients treated with fenofibrate demonstrated a significant reduction in laser treatment requirements for both diabetic macular oedema and proliferative diabetic retinopathy. The ACCORD-Eye study similarly demonstrated reduced diabetic retinopathy progression in patients receiving fenofibrate in combination with statin therapy.
Although fenofibrate is traditionally used as a lipid-modifying medication, its retinal effects are thought to extend beyond simple cholesterol reduction. Proposed mechanisms include anti-inflammatory, anti-oxidative and anti-angiogenic effects, along with possible protective effects on the retinal vasculature and blood-retinal barrier.
Importantly, fenofibrate does not replace appropriate diabetic control, retinal monitoring or ophthalmic treatment where clinically indicated. Rather, it may represent one component of broader systemic diabetic management in selected patients with diabetic retinopathy. Decisions regarding fenofibrate therapy should be made collaboratively with the patient’s general practitioner or endocrinologist, taking into account factors such as renal function, lipid profile and overall systemic health.
For health care providers wanting to learn more about the use of fenofibrate in the management of Type II diabetes, our retinal specialist Dr Neil Sharma published a review article in the Australian Journal of General Practice which can be found here.
Diabetic Retinopathy Assessment in Sydney
Eye and Retina Specialists provides assessment and management of diabetic retinopathy, diabetic macular oedema and proliferative diabetic eye disease using modern retinal imaging and treatment technologies including OCT imaging, ultra-widefield retinal photography, fluorescein angiography, retinal laser and intravitreal injection therapy.
The clinic is located in Green Square, Sydney, with patient parking available on site.