
Chalazion Surgery Sydney
Specialist Chalazion Removal, Steroid Injection and Eyelid Lump Treatment in Sydney
A chalazion is a blocked oil gland in the eyelid that can cause a firm lump, swelling, tenderness, irritation or cosmetic disturbance. Some chalazia improve with warm compresses and time, while others persist for weeks or months and may require specialist treatment.
At Eye and Retina Specialists, we assess and treat chalazion, recurrent eyelid lumps, inflamed eyelid cysts, blepharitis and related eyelid conditions. Depending on the size, duration and appearance of the lesion, treatment may include conservative care, intralesional steroid injection or chalazion surgery.
Our clinic is conveniently located in Waterloo, in the Green Square precinct, and welcomes new patient referrals from Zetland, Alexandria, Surry Hills, Mascot, Kensington, Redfern, Rosebery, the Eastern Suburbs, Inner West and greater Sydney.

Lower eyelid chalazion
What is a Chalazion?
A chalazion occurs when a Meibomian gland in the eyelid becomes blocked. These glands normally produce oil that helps stabilise the tear film and reduce evaporation of tears. When the gland outlet blocks, retained secretions and inflammation can lead to a lump forming in the eyelid.
Chalazia may occur in the upper or lower eyelid and can vary in size from small bumps to larger lesions that become noticeable or uncomfortable.
A chalazion often starts as a small lump that quickly increases in size. The contents of a chalazion include blocked fatty secretions (lipids) that normally help spread the tear film evenly and reduce evaporation.

Cross sectional diagram of a normal meibomian gland compared with a blocked meibomian gland causing a chalazion
Chalazion vs Stye – What is the Difference?
Although the terms are often used interchangeably, they are not always the same.
Chalazion
-
Usually caused by blockage and inflammation
-
Often firmer and less acutely painful
-
May persist for weeks or longer
Stye (Hordeolum)
-
Usually an acute infection near an eyelash follicle or gland
-
Often more red, tender and painful
-
May develop suddenly
Sometimes a stye can later evolve into a chalazion.
Common Symptoms of Chalazion
-
Lump in the eyelid
-
Swelling
-
Tenderness or discomfort
-
Redness
-
Heavy eyelid sensation
-
Cosmetic concern
-
Blurred vision from pressure on the eye (larger lesions)
-
Recurrent eyelid bumps
Chalazion Infection
A chalazion may become secondarily infected, and this is often associated with increased surrounding redness. If it progresses, it can lead to the more serious condition of preseptal cellulitis.
In these cases, antibiotic therapy needs to be promptly commenced. Specialist review may be needed to ensure there are no signs of the serious condition of orbital cellulitis, which needs hospitalisation and commencement of intravenous antibiotics.
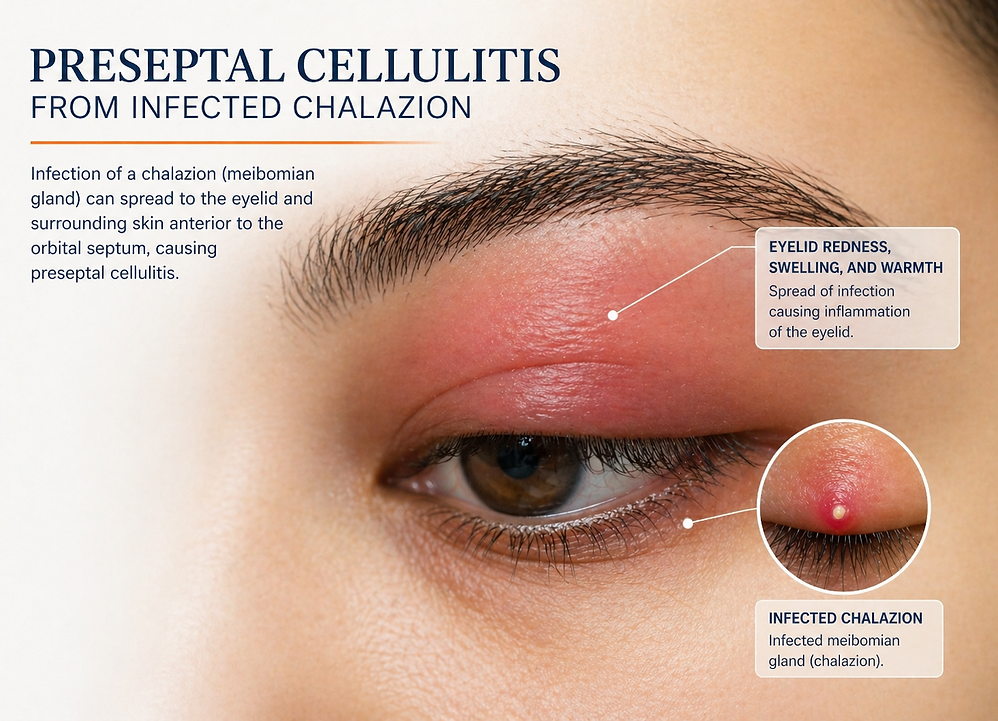
Preseptal cellulitis from infected chalazion
When is Surgical Intervention Needed?
Some chalazia may persist for longer than 4-6 weeks. If this occurs, scar tissue bands begin to form, and the chalazion is unlikely to resolve without surgical intervention. It may fluctuate in size but a residual lump usually remains.
In rare cases, a serious malignant (cancerous) lesion such as sebaceous carcinoma can mimic a chalazion.
There are two main types of intervention:
1. Intralesional Steroid Injection for Chalazion
In selected cases, an intralesional steroid injection may be considered as an alternative to surgery or alongside other treatment measures.
This involves placing a small amount of anti-inflammatory medication directly into the chalazion to help reduce inflammation and encourage the lump to resolve.
Steroid injection may be considered for:
-
Smaller or moderate chalazia
-
Multiple chalazia
-
Lesions where avoiding incision is preferred
-
Patients seeking a non-surgical option
-
Residual inflammation after partial improvement
Our specialists will advise whether your chalazion may be suitable for an intralesional injection, or if it is more likely to respond better to surgery.

Risks of Steroid Injection
Potential risks may include:
-
Skin depigmentation
-
Skin thinning
-
Raised eye pressure in susceptible patients
-
Incomplete response and need for surgery
Serious vision-threatening vascular complications have been reported with periocular steroid injections, although this is considered extremely rare. Improvement of the chalazion may occur gradually over days to weeks. Some chalazia require more than one treatment.
2. Chalazion Surgery
If a chalazion does not settle with conservative treatment, a minor procedure may be required. At Eye and Retina Specialists Sydney, we routinely perform chalazion drainage surgery in our on-site Procedure Room.
Chalazion surgery involves:
-
Topical anaesthetic drops to numb the eye
-
Anti-septic solution and sterile technique
-
Local anaesthetic to numb the area
-
Small incision (often from the inner eyelid surface)
-
Drainage / curettage of retained material
-
Division of scar tissue loculations
Ophthalmic ointment is applied, and a pad placed on the eye. We advise patients to leave the pad on for 4-6 hours after the procedure. Antibiotic eye ointment should be used twice daily for 3-5 days following the procedure. It is normal for some bruising and swelling following surgery. This normally settles within a few days.
Risks of Chalazion Surgery
Chalazion surgery is commonly performed as a minor procedure and is generally well tolerated. As with any treatment there are potential risks, including:
-
Temporary bruising, swelling, discomfort
-
Bleeding - especially if patient taking blood thinners or underlying bleeding condition. It is important to inform your doctor of this prior to surgery.
-
Infection
-
Scarring - uncommon especially if incision made through inside of eyelid
-
Incomplete resolution requiring further treatment
-
Rarely, damage to surrounding structures
Your ophthalmologist will discuss relevant risks, benefits and alternatives based on your individual situation.Our specialists are able to assess your chalazion, and recommend treatment based on the clinical appearance. If indicated, surgical incision and drainage can be performed on the same day in the procedure room in our clinic, using local anaesthetic.
Chalazion Surgery, Sydney
Frequently Asked Questions (FAQ)
Q1. What is a chalazion?
A chalazion is an eyelid swelling characterised by chronic, lipogranulomatous inflammation originating from a blocked Meibomian gland orifice.
Q2. What age do chalazion occur?
Chalazion can occur at any age. In the elderly in particular, it is important to ensure a chronic chalazion is not misdiagnosed as the rare but serious malignancy called sebaceous carcinoma.
Q3. Are there predisposing factors?
A chalazion can develop in anyone. People with blepharitis and acne rosacea are at a higher risk. Chalazia may be more common in people who work in dusty environments, people with incomplete makeup removal and people with diabetes.
Q4. What is the initial management of a chalazion ?
Regular hot compress and massage over the lump done regularly, especially in the first four weeks or until the lump discharges and resolves. Oral antibiotics are only required if there is associated eyelid infection (preseptal cellulitis).
We recommend patient's continue hot compress and massage of the eyelid at least once daily for 6 months following a chalazion, to reduce the risk of further chalazia developing. If there is underlying blepharitis, the hot compress and massage should ideally be continued indefinitely.
Q6. How do I prevent further chalazia?
